Effects of exercise on tests measuring attention and executive function in younger and older adults
Article information
Abstract
Purpose
This study investigated whether or not performance differed between Young and Older Exercisers and between Young and Older Non-exercisers on the Attention Processing Training-Test (APT-Test), Behavioral Assessment of Dysexecutive Syndrome (BADS), and Functional Assessment of Verbal Reasoning and Executive Strategies (FAVRES).
Methods
A total of 119 participants were divided into the following groups: 46 Young Exercisers: (aged 18–40 years), 45 Older Exercisers (aged 60 and older), fourteen Young Non-exercisers, and fourteen Older Non-exercisers. Participants completed the APT-Test, BADS, and FAVRES in a counterbalanced manner. Independent sample t-tests were used to calculate outcomes.
Results
Young Exercisers had significantly higher scores than Older Exercisers on the APT-Test, BADS Total Profile Score, and the FAVRES Total Accuracy Score. No significant differences occurred between Young and Older Exercisers on the FAVRES Total Rationale, Total Time, or Reasoning scores. No statistically significant differences occurred on any measures between Young and Older Non-exercisers.
Conclusions
Different performance trends occurred between the Exerciser groups and the Non-exerciser groups. For example, both Exerciser groups performed similarly on the FAVRES when asked to justify their responses and perform reasoning tasks. Older Exercisers provided correct responses for Accuracy measures, yet their responses did not earn the total points. No differences occurred on any test between the Non-exerciser groups. Thus, it could be helpful for clinicians to inquire about patients’ pre-morbid exercise habits when using these tests. Participants were healthy, neurologically intact adults. Future research should investigate potential effects exercise has on these tests in adults with acquired neurological damage.
INTRODUCTION
Researchers have studied the effects of physical activity and measures of attention and executive function (EF) in adults across the lifespan. EF is a broad term that encompasses various complex cognitive processes used to analyze and assign meaning to incoming information, and these processes are often responsible for behaviors such as initiating, planning, organizing, sequencing, switching, inhibiting, and problem solving [1–7]. Having adequate EF allows individuals to competently function in daily life by assessing new incoming information, use prior knowledge from past experiences to analyze the current situation, determine a plan of action, and then reflect on the consequences [3,5,7,8]. EF disruptions can negatively impact decision making and self-control, leading to inappropriate behaviors and the inability to perform daily living skills. Thus, EF enables individuals to lead independent, fulfilling lives [1,5,8,9].
Attention enables individuals to focus on relevant information and is comprised of several different types, including alternating attention in which individuals rapidly shift this focus amongst various stimuli, selective attention in which certain stimuli are focused on while others are not, and sustained attention in which target stimuli are focused on for an extended period of time [1,7,10,11]. Attentional skills allow persons to filter out irrelevant incoming information and focus on essential information to complete desired tasks [1,7,10,12]. EF and attention are posited to be interconnected and integrated cognitive mechanisms; the inability to focus our attention on relevant information leads to EF disruption [1,4,10,12]. Previous research studies have determined a relationship between aging and poor performance on cognitive measures [13–15]. Younan [16] suggests that age-related cognitive decline can result in decreased “processing speed, reasoning skills, memory, and executive functions.” As individuals age, structures can display significant deterioration and undergo a reduction in neural connections that are necessary for advanced cognition skills like EF and attention. For instance, the hippocampus and frontal lobe experience a significant decline in functioning due to aging [9,15]. Aerobic exercise has been found to increase volume in the gray and white matter within the frontal and temporal lobes to preserve cognitive processes involved with attention and EF [14,15,17]. Therefore, exercise is a simple and inexpensive activity that could decrease the cognitive effects related to aging and positively impact performance on EF and attention tasks [17].
Many factors contribute to persons having robust cognitive skills during their lifetime, including the aforementioned engaging in exercise [16,18,19]. For example, Hawkins, Kramer, and Capaldi found that older adult exercisers had significantly better performance on dual attention tasks than older adult non-exercisers [20]. Yaffee et al. [21] reported that participants aged 65 and older who exercised had less risk of having cognitive declines, and that the more older adults exercised, the less likely they were to develop cognitive declines later in life. Eggemont et al. [18] had participants complete an activity questionnaire as well as various EF and cognitive tests. Older adult participants who were more physically active, including those who exercised, had higher scores on all EF and cognitive measures versus older adults who were not as physically active [18]. More recently, young adults in a high physical activity group, which included exercise, had significantly higher EF measures versus young adults in a low physical activity/exercise group [22]. Lower levels of physical activity and exercise in 4,555 adults aged 50 and older followed for six years correlated with lower verbal fluency and letter cancellation scores; participants with higher physical activity levels also had better EF [23]. Thus, persons across the lifespan who exercise can have higher scores on attention and EF measures.
There are many factors to consider when discussing the broad term of “exercise.” “Exercise” can often be synonymous with “physical activity” [24,25], yet researchers have attempted to define differences between the terms. Being engaged in physical activities can be subjective, and vary across individuals and at various points in their lives [24], however, the type of physical activity, the intensity of physical activity, and the duration of physical activity can have different impacts on cognition [25]. Household tasks (e.g., yardwork, cleaning, home repair) can be considered physical activities, some of which can require significant exertion. Tools such as the Physical Activity Scale for the Elderly (PASE) can be used to determine older adults’ physical activity by asking questions regarding their participation in activities such as sitting (e.g., reading, watching TV), walking, light sport or recreational activities (e.g., bowling, fishing), moderate sport or recreational activities (e.g., golfing without a golf cart, ice skating), and strenuous sport or recreational activities (e.g., jogging, swimming) [26]. Exercise has been defined as “physical activity that is planned, structured, repetitive, and purposive in the sense that improvement or maintenance of one or more components of physical fitness is an objective” [24]. McKinney et al. [27]. defined exercisers as individuals whose primary goals are to be healthy and fit and who exercise more than 2.5 hours of the week. Previous research studies investigating cognition have developed various criteria for both the inclusion of participants and separating participants into different groups based on the above noted factors (i.e., type, intensity, and duration of exercise) [28]. Erickson et al. [15] randomly assigned participants into either an aerobic or a stretching and toning exercising group, while Colcombe et al. had all participants attend 1-hour exercise programs, three days a week [14].
Tests used in the current study have been described in previous studies [13,29–31]. The Attention Process Training Test (APT-Test) evaluates simple sustained, complex sustained, selective, divided, and alternating attention [32]. Researchers read aloud the instructions and played a CD for each of the five subtests (i.e., levels) in which numbers are read aloud; levels increased in difficulty. Persons press a clicker when they hear a correct response (e.g., a number that is one less than the number immediately prior to it during the complex sustained attention subtest). For level 1, the simple sustained attention subtest, individuals press the clicker when they hear the number “two” read aloud. As previously described, participants click when they hear a number that is one less than the number right before it for Level 2, the complex sustained subtest. Participants press the clicker when they hear the number “two” while random words are being said aloud in the background during level 3, the selective attention subtest. For the divided attention task (level 4), participants click when they hear the number “two” while simultaneously using a pen or pencil to cross off even numbers (e.g., 2, 4, 6) in a display of numbers on a 8 ½”×11” piece of paper. For level 5, alternating attention and the last task, persons click when they hear a number that is one less than the number right before it. When the researcher says “switch” during the audio presentation, participants then have to click when hearing a number that is one more than the number immediately prior to it. Switching events occur numerous times. The test manual states that administration takes approximately 20–30 minutes, and reports normative data for an original sample of 25 control individuals (Mage=26.3) and 25 persons with mild brain injuries (Mage= 27.2). Means and standard deviations for the age groups of 18–29 years, 30–39 years, 40–59 years, and 60–85 years old are also reported [32].
Both EF tests used in the current study have also been described by researchers [13,29,31]. The Behavioural Assessment of the Dysexecutive Syndrome (BADS) [33] includes six tests (i.e., subtests) to assess EF abilities. Verbal, written, and hands-on responses are required. In the first test, persons quickly learn one rule pertaining to a set of playing cards (e.g., hearts, spades), perform the target task, quickly unlearn the original rule and learn a new rule, then complete the task using the new rule. Examples of other tests participants complete include responding to temporal judgement questions (e.g., How long does it take to blow up a party balloon?), mapping out paths to zoo exhibits per specific rules, and drawing how they would look for lost keys in a field. The examiners manual reports the test can be given in 40–50 minutes and was normed on 216 healthy adults divided into four age groups: 16–31, 32–47, 48–63, 64 years and older, as well as on 78 individuals (aged 19–78) with neurological disorders [33].
For the Functional Assessment of Verbal Reasoning and Executive Strategies (FAVRES) [34], participants are administered four subtests and provide verbal and written responses. Subtests include, but are not limited to: finding a suitable birthday activity for a young male relative based on a list of available activities, budget constraints, and schedule. Another subtest requires individuals to schedule a workday when given a list of tasks that need to be done, some of which are higher priority than others. Participants also complete prediction and generation tasks for each subtest (e.g., what good and bad things could happen from meeting with an angry customer; generate as many ways to advertise as possible). The FAVRES takes generally 50–60 minutes to give and was normed on 101 healthy persons aged 17–89 years and 52 adults with acquired brain injury [34,35]. Both the BADS and FAVRES are ecologically valid tests speech-language pathologists (SLPs) could give their adult neurogenic patients [35,36].
The APT-Test [32], BADS [33], and FAVRES [34] have been used across several research studies to measure EF and attention [3,8,13,29–31,35,37–40]. Johnston recently conducted a survey that included 51 practicing speech-language pathologists (SLPs) who developed a list of formalized assessments administered to evaluate their adult patients’ cognition [41]. The relative frequency of usage of the APT-Test [32], BADS [33], and FAVRES [34] was estimated based on responses in the survey. The FAVRES [34] was listed by 32% percent of SLPs as a formalized assessment commonly administered to their patients and was rated as the second most popular assessment used to evaluate cognition [41]. The APT-Test [32] and BADS [33] were also listed in the top 20 cognitive assessments used by practicing SLPs. Other studies investigating the effects of physical activity or exercise on aspects of cognition have used differing cognitive tests [18,42], such as the Trailmaking Test (TMT) [43], the Hopkins Verbal Learning Test-Revised (HVLT-R) [44], and the Clock-in-a-Box Test (CIB) [45]. However, based on the data gathered from Johnston’s [41] survey, such tests are not used by clinicians working in the field [41]. Rather, the APT-Test [32], BADS [33], and FAVRES [34] are common formalized assessments administered by practicing SLPs [41].
Despite such research, more information is needed. The lack of research on the effects of exercise on attention and EF tests that SLPs may give their adult patients makes it essential to further explore any potential relationship. In addition, no studies have been found in which attention and EF test scores on these specific assessments have been compared between older and younger adult exercisers and older and younger adult non-exercisers, respectively. Determining if exercise has an effect on these tests’ scores contributes to the literature base and may add to the information SLPs would want to obtain from their patients and/or patients’ family members and caregivers. The following research questions were addressed: 1) Are there performance differences on the APT-Test [32], the BADS [33], and the FAVRES [34] between younger and older adult Exercisers? 2) Are there performance differences on the APT-Test [32], the BADS [33], and the FAVRES [34] between younger and older adult Non-Exercisers?
METHODS
Participants
The participants for this cross sectional quasi-experimental study were approved by the University of Northern Iowa’s Institutional Review Board (Protocol # 19–0125). Participants were recruited from small, mid-sized, and large metropolitan communities and from rural areas in the Midwest by posting flyers in public areas (e.g., community centers). Similar to prior studies [13,29,30], inclusion criteria included: no neurological impairment or disorders; be a native English speaker; minimum of a high school education; score of 28 or higher on the Mini-Mental State Examination (MMSE) [46]. Upon meeting inclusion criteria, participants were asked to report whether or not they exercised. Those who indicated they did were classified as Exercisers, which were specifically defined as individuals who engaged in various physical activities a minimum of three times per week in order to improve or maintain their fitness and health [27]. Exercisers were asked to report on average, how frequently during the week they exercised, and what kinds of physical activities they partook in. For the purpose of this study, acceptable physical activities included walking, swimming, running, jogging, biking, lifting weights, attending a workout class, and/or doing yoga [23, 27,47]; housework and yard work were not considered “exercise” [24]. Participants who reported they did not exercise were categorized as Non-exercisers. A power analysis for an effect size of .08 with an alpha of .05 indicated that a minimum of 105 participants was necessary. A total of 119 adults participated and were broken down into the following groups: 46 Young Exercisers: (aged 18–40 years), 45 Older Exercisers (aged 60 and older), fourteen Young Non-exercisers, and fourteen Older Non-exercisers. Age groups were defined based on prior studies [13,29]. Table 1 includes mean ages and mean MMSE scores for the four participant groups.

Mean Age and MMSE Scores
Stimuli, Procedures, and Data Analysis
Once individuals met all inclusion criteria and responded to the questions about exercising, participants completed an individual session in which the APT-Test [32], BADS [33], and FAVRES [34] were administered in a counterbalanced order. Length of sessions generally ranged from 90–120 minutes with breaks provided. Although hearing screenings were not conducted [35], researchers presented directions at a comfortable volume level and adjusted their volume, if necessary.
Data analysis was similar to prior studies [3,8,13,29,31,48]. Overall total test scores for the BADS and FAVRES were used for analyses. For the APT-Test [32], no overall test score was calculated. Thus, Residual Scores (i.e., total responses correct) were reported for each of the five APT-Test [32] subtests: sustained, complex sustained, selective, divided and alternating. The possible maximum score was 24 for the alternating attention subtest; the total score possible for the other four subtests was 30. For the BADS [33], an overall Total Profile Score ranging from 0–24 was obtained by adding up the Profile Scores from each of the six tests (i.e., subtests). For the FAVRES [34], participants obtained the maximum points possible if they provided responses containing the most pieces of correct information; some points were given if they provided responses that were sufficient but lacked all of the necessary pieces. Raw scores were converted into Total Standard Scores for Accuracy, Rationale, Time, and Reasoning (M=100, SD=15). As noted by Kelkar, Hough, and Fang, higher Accuracy, Rationale and Reasoning scores indicated better participant performance; higher scores on Timing indicate poorer performance (i.e., target task took longer) [48].
Reliability
Pearson r correlations were calculated using raw scores on 20% of a randomly chosen sample (i.e., 24 participants). The researchers and a trained graduate speech-language pathology student’s scores were correlated for inter-rater reliability. The researchers scored the protocols twice for intra-rater reliability; the second scoring took place four weeks following the initial scoring. Inter-rater reliability for the APT was r=0.90; intra-rater reliability was r=0.92. Inter-rater reliability for the BADS was r=0.88; intra-rater reliability was r=0.94. Inter-rater reliability for the FAVRES was r=0.89; intra-rater reliability was r=0.95.
RESULTS
Descriptive statistics
Overall mean scores were obtained for each test (Table 2). As previously noted, residual scores for each subtest on the APT-Test were calculated since no overall total score is obtained. The Total Profile Score was obtained for the BADS, and Total Accuracy, Total Rationale, Total Timing, and Reasoning Standard Scores were calculated for the FAVRES. Older Exercisers had lower mean scores on all three tests compared to Younger Exercisers. Older Non-exercisers had slightly higher scores on the APT-Test’s Sustained Attention subtest and higher mean scores on the FAVRES’ Total Accuracy score versus Young Non-exercisers.
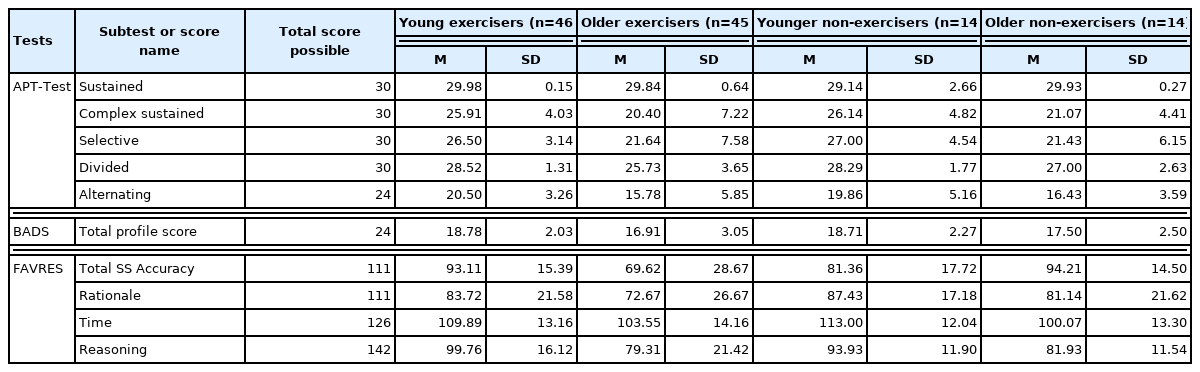
Mean APT-Test, BADS, and FAVRES Scores
Inferential statistics
Independent sample t-tests were conducted to determine if statistically significant differences occurred between Young and Older Exercisers and between Young and Older Non-exercisers.
Exercisers
Statistically significant differences occurred between Young and Older Exercisers on all APT-Test subtests: Sustained Attention (t(89) 1.39, p≤0.007), Complex Sustained Attention (t(89)= 4.51, p≤0.0001), Selective Attention (t(89)=4.01, p≤0.0001), Divided Attention (t(89)=4.87, p≤0.0001), and Alternating Attention (t(89)=4.77, p≤0.003). Young Exercisers also had statistically higher scores on the BADS Total Profile Score (t(89)= 3.45, p≤0.015) and FAVRES Total Accuracy score (t(89)=4.88, p≤0.0001) versus Older Exercisers. No statistically significant differences occurred between the two groups on the following FAVRES scores: Total Rationale (t(89)=2.18, p>0.39), Total Time (t(89)=2.20, p>0.48), and Reasoning (t(89)=5.15, p>0.30) (Table 3).
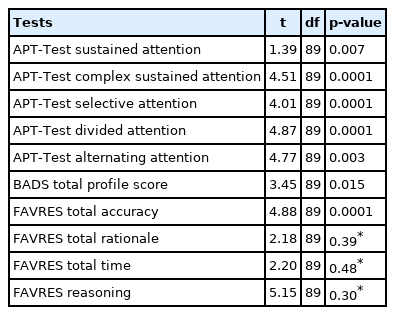
Exercisers’ Independent Samples t-test Results for APT-Test, BADS, and FAVRES
Non-Exercisers
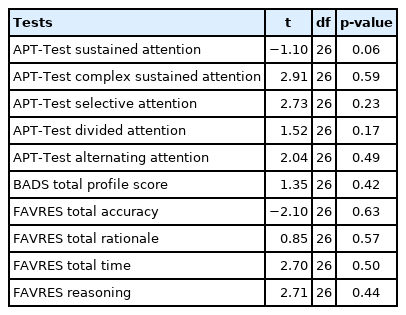
No statistically significant differences occurred between Younger and Older Non-exercisers on any of the three tests. More specifically, no statistically significant differences occurred on any of the APT-Test subtests: Sustained Attention (t(26)=−1.10, p>0.06), Complex Sustained Attention (t(26)=2.91, p>0.59), Selective Attention (t(26)=2.73, p>0.23), Divided Attention (t(26)=1.52, p>0.17), and Alternating Attention (t(26)= 2.04, p>0.49). Also, no statistically significant differences occurred between both Non-exerciser groups on the BADS Total Profile Score (t(26)= 1.35, p>0.42) or on the following FAVRES scores: Total Accuracy (t(26)=−2.10, p>0.63), Total Rationale (t(26)= 0.85, p>0.57), Total Time (t(26)=2.70, p>0.50), and Reasoning (t(26)=2.71, p>0.44) (Table 4).
DISCUSSION
This study sought to determine if performance differences occurred on the APT-Test [32], the BADS [33], and the FAVRES [34] between Young and Older Exercisers and between Young and Older Non-exercisers, respectively. Young Exercisers had significantly higher scores versus Older Exercisers on the APT-Test, the BADS Total Profile Score, and the FAVRES Total Accuracy Score. No significant differences occurred between Young and Older Exercisers on the FAVRES Total Rationale, Total Time, or Reasoning scores. No statistically significant differences occurred on any measures between the Young Non-exercisers and Older Non-exercisers. Younger adults having higher scores than older adults on the APT-Test, BADS, and FAVRES has been documented [13,38]. In addition, data indicate that in general, older adults can have poorer performance on attention and executive function scores versus younger adults [14,15]. Researchers have also reported that physically active adults have higher attention and executive function scores than those who are not as physically active [18,20–23]. This is the first known study to compare the performance on tests SLPs may use between younger and older adults who exercise as well as between younger and older adults who do not exercise.
As noted, although Young Exercisers and Older Exercisers had differences on several scores (i.e., APT-Test, BADS Total Profile Score, FAVRES Accuracy), they did not evidence any statistically significant difference on the FAVRES’ Rationale, Time, or Reasoning Scores. This suggests that overall, the two groups of exercisers performed generally similarly when asked to provide justifications for the responses they chose, that they took a similar amount of time to complete the various tasks, and they were able to adequately perform generating and predicting tasks. Tasks on the FAVRES [34] much more closely resemble that of activities found in everyday life. Persons do not necessarily press a clicker when listening for target numbers in a string of numbers with changing rules, such as those found in the APT-Test [32], nor do they tend to complete worksheets denoting which paths they would take when searching for keys or visiting exhibits, or verbally respond to quickly changing rules regarding playing cards, such as those tasks found in the BADS [33]. However, similar to tasks in the FAVRES [34], most individuals must plan their day, prioritize what is important and must be dealt with sooner rather than later, and manage when unexpected circumstances arise. Persons may also find themselves at some point in time needing to complain or have concerns about a repair not being done correctly. Thus, tasks in this test more closely resemble that of everyday life and are more ecologically valid in nature [34].
While there were statistically significant differences on the FAVRES’ Total Accuracy score, Older Exercisers still generally provided accurate responses. The issue is that Older Exerciser participants did not provide responses in which they earned the highest points possible for Accuracy. This trend was reported in a prior study in which South Asian adults choose correct responses, but also did not provide responses in which they earned the highest points compared to White adult participants [31]. Thus, Older Exercisers’ responses were not necessarily incorrect per se, but rather lacked all of the target information that would have led to higher scores. As noted in Kallambettu, Burda, and Wakeman, instructions given to the participants do not state that choosing or providing specific responses will lead to participants earning the highest points possible [31]. It is possible that the Older Exercisers would have had higher scores had more explicit test directions denoted that more pieces of correct information would have led to higher scores. Nonetheless, Older Exercisers were just as successful as Young Exercisers when providing rationales for their chosen answer and when asked to provide generating and predictive responses (i.e., Reasoning scores). This is not necessarily surprising as older adults can have equally robust problem solving and reasoning skills as younger adults, particularly for scenarios that are more daily life oriented [49–51]. However, researchers are not necessarily in agreement if older adults do well in more ecologically-based problem solving research tasks simply because they have more years of real world experience [50]. Prior studies have also found that older adults generally take longer on the FAVRES’ than younger adults [13,38], yet no Time differences occurred in the current study. Older adults can be efficient problem solvers [51], and it is conceivable the ecologically valid tasks on the FAVRES may have minimized any potential performance differences between the two differently-aged Exerciser groups [52].
It is interesting no differences occurred between Young Exercisers and Older Non-exercisers. This was somewhat unexpected as prior studies noted above have shown performance differences on measures of attention or executive function with respect to age [13,15,38] and physical activity [18,20,22, 23]. However, Younan recently investigated potential performance differences in EF scores in young-old adult exercisers, old-old adult exercisers, young-old sedentary adults, and old-old sedentary adults [16]. While young-old adults (aged 45–67) consistently scored better in digit span and latency tasks than old-old adults (aged 72–94) regardless of activity level, the old-old adult exercisers scored worse on latency measures than old-old sedentary adults. No significant differences occurred amongst the different groups on the Wisconsin card-sorting task [16]. Although younger adults were not part of the Younan study, results from that study indicate that it is possible there may be no performance differences on certain cognitive measures, regardless if individuals exercise [16]. SLPs may not typically ask patients about exercise habits when using the APT-Test [32], BADS [33], or FAVRES [34], however, the current study suggests it is plausible such inquiries should be made to better gain an overall understanding of patients’ pre-morbid functioning.
Limitations and future research
There are several limitations with this study. First, participants self-reported whether or not they exercised. Although other researchers have obtained participant self reports on exercise [18,21,22], objective data has also been obtained (e.g., accelerometer; number of steps per day) [19,22,47]. Also, older adults’ self-reports of physical activity may differ from their actual physical activity [49]. The current study asked participants to report whether or not they exercised and to report on the amount; they were not asked to report the intensity of exercise (e.g., light, moderate), yet older adults’ exercise may differ in its intensity compared to younger adults [47]. In addition, participants were not asked to document their overall physical activity. Some household activities and yardwork could be similar to exercise (e.g., washing windows, splitting and stacking wood). Participants may not have been considered formal exercisers, yet were quite physically active. Therefore, the activities the researchers considered “exercise” may have not truly captured the degree of physical fitness that participants possessed. Another limitation is that the study only took into account whether or not participants were exercising at the time of the study. Other variables were not included as part of the data analysis, such as whether or not participants smoked [53] or if they were involved in some kind of socially engaging activities either through work or volunteering [54, 55]. Their verbal and non-verbal intelligence abilities were not tested, yet all of these factors have been found to have implications on adults’ cognitive functioning [56,57].
Age group classifications were based on prior research studies [13,30,58]. However, age groupings have been variable in prior studies relating to aging, cognition, and also exercise [15,16,22,23,38,59]. Only three participants were in their 80s, none were in their 90s; the majority of Older Exercisers and Older Non-exercisers participants were in their 60s. Yet, some researchers have reported that real world problem solving may decline in adults over the age of 75 [60]. It is possible that including more individuals in their 80s and 90s, perhaps even as a stand alone group, would have yielded different results. In addition, all participants were neurologically intact. It is difficult to fully understand possible clinical implications exercise may have on individuals’ scores on the tests used in this study until acquired neurological damage is present.
Future research should include replicating this study using objective measures in addition to self reports. Including measures of intensity and/or questionnaires, such as the Physical Activity Scale for the Elderly (PASE) [61] or Paffenberger Physical Activity Questionnaire [62] could also be beneficial. In addition, it would be helpful to include participant groups representing more diverse age groups. This study consisted of healthy adult participants. However, obtaining data on the premorbid exercise habits of persons with acquired neurogenic communication disorders could inform SLPs if asking about exercise habits is of particular clinical value when administering any of the tests used in this study.
ACKNOWLEDGMENTS
This study was presented November 2019 at the Annual Meeting of the American Speech-Language-Hearing Association in Orlando, Florida.