Patient and caregiver satisfaction regarding telepractice versus in-person services at a university speech, language, and hearing clinic
Article information
Abstract
Purpose
The purpose of the pilot study is to explore patient and caregiver (i.e., spouse, parent, grandparent, child, and grandchild) satisfaction regarding telepractice versus in-person services provided at a university speech, language, and hearing clinic.
Methods
Survey data were collected from 70 respondents (24 received in-person services only, 13 received telepractice only, and 33 received both in-person services and telepractice) during the onset of the COVID-19 pandemic.
Results
Results indicated that patients and caregivers rated overall in-person services significantly higher than the overall telepractice services. Patients’ and caregivers’ perceived technology skills were not significantly related to their satisfaction of telepractice. However, graduate clinicians’ technology skills, professionalism, and the quality of materials used in sessions were significantly associated with patients’ and caregivers’ satisfaction of telepractice. Also, patients’ and caregivers’ interaction with graduate students and supervisors was significantly correlated to their satisfaction of telepractice.
Conclusions
Areas of improvement for telepractice-based services were discussed. The significance of adopting telepractice clinical and technical skills in preservice speech-language pathology pedagogy was also highlighted.
INTRODUCTION
In the spring of 2020, the COVID-19 pandemic created conditions in which required significant changes to clinical service delivery. Many university clinics elected to migrate to a telepractice-focused model of clinical service delivery. This created opportunities and challenges for any university clinic. The current study examines preliminary data regarding patient and caregiver satisfaction on the rapid conversion of service delivery from conventional in-person services to telepractice during this period. The purpose of the pilot study is to survey the satisfaction of patients and caregivers regarding in-person services versus telepractice provided at the university speech, language, and hearing clinic. Surveying service modality across these populations can be beneficial to advance knowledge of service delivery methods. At the host university clinical setting, in-person service delivery had been the predominant method provided to patients. Thus, graduate students had historically provided in-person services because their undergraduate and graduate coursework and graduate clinical training heavily focused on the in-person service delivery model until the spring 2020 semester. During the global pandemic, when conventional in-person services were prohibited, videoconference-based telepractice was the one and only service delivery model that practitioners and patients were allowed to participate in safely. Converting to a telepractice-based model of service delivery has both benefits and challenges to providers and patients. From a provider standpoint, this modality was a completely new model of service delivery, with little training provided didactically. For patients and caregivers, telepractice may provide increased convenience, as they would not have to travel onsite to a clinic to receive services. However, limitations such as inconsistent or interrupted internet services can present as a significant barrier towards receiving services. Given that the graduate clinicians and supervisors were not fully trained and prepared in implementing telepractice, the researchers surveyed if patients and caregivers were satisfied with telepractice services compared to in-person services. Examining patients’ and caregivers’ satisfaction, as a measure to determine the effectiveness of the quality of service, may help university faculty and clinical supervisors identify areas of improvement for telepractice-based services and clinical education.
Telepractice versus in-person service delivery
Telepractice refers to the use of telecommunication technology for the delivery of speech-language pathology and audiology services at a distance by connecting a clinician to a patient for diagnostic, therapeutic, and consulting services [1]. ASHA indicates that telepractice is an appropriate model of service delivery for audiologists and speech-language pathologists [1]. Telepractice is a simple but powerful strategy to continue service delivery while eliminating infection risk by avoiding in-person contact between patients and healthcare professionals [2]. Researchers have attempted to demonstrate the effectiveness of telepractice, compared with in-person modality, on individuals with a variety of communication disorders by using treatment outcomes as dependent variables. For example, Brennan et al. [3] examined the effects of videoconference-based interaction between a clinician and a patient with a brain injury, compared to in-person modality, on story retelling tasks. Results revealed no differences and high correlation between telepractice and in-person modality in accuracy of story retelling. Age, education, technology experience, and gender did not influence the difference between performance in the two settings. Mashima et al. [4] studied if voice therapy could be delivered effectively via telepractice. No differences in outcome measures (i.e., perceptual judgments of voice quality, acoustic analyses of voice, patient satisfaction ratings, and fiber-optic laryngoscopy) were found between the in-person group and the telepractice group.
Grogan-Johnson et al. [5] investigated whether school-age children with speech sound impairments could demonstrate improvements in accurate production of targeted sounds via telepractice compared with in-person modality. It was found that children in both modalities exhibited progress in their speech sound production during the program. No significant differences were found between the two conditions on post-intervention. Wales et al. [6] conducted a systematic review to determine whether speech-language pathology interventions via telepractice are as effective as traditional in-person delivery for school-age children with speech and/or language impairments. Although the amount of research was limited and the quality of reviewed studies varied, results revealed that participants in both telepractice and in-person conditions made significant and similar improvements.
In summary, evidence demonstrates that telepractice using videoconferencing software, which allows a patient and a clinician to see and hear each other, is a feasible, promising, and effective model of service delivery for both clinician and client compared to in-person modality. It is noteworthy that the reviewed empirical studies defined telepractice as real-time or synchronous videoconference-based technology. Network connection speed, technology compatibility, and patients’ confidentiality must be basic requirements for successful implementation of telepractice.
Patient and caregiver satisfaction
Patient satisfaction is a critical component for measuring the quality of healthcare services, given the importance of patient-centered care [7]. The main purpose of patient satisfaction surveys is to improve the delivery of healthcare services by understanding provided services’ strengths and weaknesses from the patient perspective [8]. Patient satisfaction surveys tend to be the primary method of quantifying patient satisfaction to determine the efficacy of the quality of telepractice. For example, Crutchley and Campbell [9] surveyed the satisfaction of parents/guardians, teachers, and administrators with a year-long school-based telepractice delivered by a university clinic in a rural, remote county of North Carolina. Overall satisfaction with the videoconference-based telepractice program was found across stakeholders. However, not all parents/guardians and teachers were satisfied with telepractice. Connectivity (e.g., a Wi-Fi environment and available bandwidth) is found to be related to the satisfaction of patients. For example, Jahromi and Ahmadian [10] assessed the satisfaction of patients with stuttering, aged between 14 and 38 years, in videoconference-based telepractice services and the infrastructure for the implementation of telepractice in Iran. Results indicated no significant relationship between the patients’ satisfaction and their gender, education level, and age. Overall, patients were satisfied with telepractice services, but the low speed of the internet connection in the country was a major challenge for receiving telepractice services.
Polinski et al. [11] conducted a paper-based survey to study whether CVS Pharmacy Minute Clinic’s videoconference-based telepractice option satisfied patients’ health care needs. In total, 1,734 (54%) of 3,303 patients reported high satisfaction (i.e., better than or as good as conventional in-person services) with their telepractice experience specifically citing the quality of care received, and telepractice’s convenience as primary reasons for their satisfaction. Kruse et al. [12] completed a systemic review to examine the relationship between telepractice and patient satisfaction and found that top five factors in choosing telepractice services include improved outcomes, preferred modality, ease of use, low cost or cost savings, and improved communication.
Recent studies reported patient satisfaction concerning telepractice services during the COVID-19 pandemic when conventional in-person services are limited or prohibited. For example, Tedforde et al. [13] conducted an online survey to measure patient satisfaction of telepractice services (i.e., outpatient physical, occupational, and speech-language therapy synchronous telepractice) during the COVID-19 pandemic. Results indicated that those who identify as female participated in telepractice sessions more frequently and provided higher ratings than those who identify as male. Patients and patient care advocates reported high quality healthcare delivery for all patient-centered outcome metrics. Benefits identified by the respondents included no travel time, possible collaboration with other healthcare advocates, and convenience of service delivery. Limitations included technology barriers and limited hands-on experiences.
Lam et al. [14] evaluated students’ and parents’ perceptions of telepractice efficacy and their preferences for different service delivery models during the COVID-19 pandemic in Hong Kong. Both students and parents were satisfied with telepractice services but believed telepractice was less effective than the conventional in-person practices. Parents preferred in-person services over the telepractice, whereas students did not prefer one mode of practice over the other. Fieux et al. [2] investigated patient satisfaction concerning otolaryngologists’ consultation via videoconference-based telepractice during the COVID-19 in France. It was found that overall patient satisfaction of telepractice consultation was high. Two negative predictors with satisfaction included the absence of physical examination and poor sound and video quality.
In sum, cumulated evidence concludes that overall patients and stakeholders are satisfied with the effectiveness and efficacy of videoconference-based telepractice services. Telepractice services do not allow complete and comprehensive healthcare services but the above demonstrate that they are well accepted by patients.
Telepractice-based clinical education
Given the importance and popularity of telepractice in speech-language pathology, speech-language pathology graduate students should obtain the skills and knowledge competencies needed for telepractice [15]. However, a significant gap between the need for preservice telepractice training and actual implementation of telepractice instruction has been reported. For example, Grogan-Johnson et al. [5] surveyed program coordinators in speech-language pathology graduate programs to describe preservice telepractice training at the university level. Most respondents indicated that telepractice applications should be taught to speech-language pathology graduate students, but only 26% of the programs provided telepractice instruction.
Overby [16] surveyed faculty, speech-language pathology graduate students, and telepractice practitioners to identify (1) effective teaching strategies for preservice telepractice training, (2) key components of telepractice clinical instruction, and (3) barriers to adopting telepractice in preservice training. All groups ranked hands-on training (e.g., demonstrations of telepractice, practice, and role playing) as the most effective method for telepractice instruction. It was also found that telepractice clinical skills (e.g., appropriate selection and preparation of online materials, interpersonal skills, and remote behavior management) were ranked the most important aspect of preservice telepractice training, followed by telepractice technology skills and knowledge of legal issues. Identified barriers among the respondents included (1) difficulty finding appropriate online telepractice materials, (2) managing technology problems, and (3) establishing rapport with patients.
In summary, evidence highlighting the importance of preservice telepractice training is emerging. Faculty and practitioners agree that preservice telepractice instruction is critical for preparing speech-language pathology graduate students for entry-level competences in telepractice. Preliminary data suggested pedagogical strategies and key components as well as challenges in adopting telepractice in graduate curriculum. More empirical investigations in preservice telepractice instruction are necessary to promote the preparation of speech-language pathology graduate students.
Purpose of the present study
Research indicates that videoconference-based telepractice, which allows a patient and a clinician to see and hear each other, is a feasible, promising, and effective model of service delivery compared to in-person modality. Given the importance and popularity of telepractice, implementing telepractice instruction in speech-language pathology graduate programs is emerging.
Within the researchers’ host university, 33 first-year speech-language pathology graduate students who participated in their first in-house practicum at the university clinic were required to convert clinical service delivery from in-person modality into videoconference-based telepractice via Zoom teleconferencing software. Clinical supervisors who are certified and licensed speech-language pathologists and audiologists had to quickly adapt to this transformation without proper training and experience. Conversions that would typically take months of planning, pilot testing, revision, and training of clinical supervisors and graduate students had been completed into two weeks. Both graduate clinicians and supervisors continued to provide telepractice services to their patients and caregivers in the summer 2020 semester due to continuous safety concerns. The purpose of the current pilot study is to collect initial insights into patients’ and caregivers’ satisfaction of telepractice versus in-person services provided at a university speech, language, and hearing clinic. The association between patients’ and caregivers’ satisfaction of telepractice and graduate students’ clinical and technology skills in telepractice was especially targeted. Careful examination of patients’ and caregivers’ satisfaction, as a measure to determine the effectiveness of the quality of service, may shed light on identifying areas of improvement for telepractice-based services and clinical education.
METHODS
Participants
A survey was distributed in October 2020 to 160 families who received speech, language, and hearing services at a university clinic in fall 2019 (in-person only), spring 2020 (both in-person and telepractice), and/or summer 2020 (telepractice only). Prior to beginning services, patients and caregivers who received remote clinical service agreed that (1) they are responsible for videoconferencing tools (i.e., hardware, software, and peripheral devices) as well as internet services (e.g., Wi-Fi), (2) they receive telepractice in a private room in their home, free from distractions, and (3) a pediatric patient or an adult patient requiring facilitation and/or technology assistance has a support person in the room all times. The clinic’s administrative assistant identified the 160 families, and one person, either patient or caregiver (i.e., spouse, parent, grandparent, child, and grandchild) listed as the main contact in each family. Those identified as a potential participant received a survey created through Qualtrics survey software via email to describe their satisfaction of speech, language, and hearing services provided at the university clinic. This study was reviewed and approved by the Institutional Review Board prior to data collection and analysis.
Questionnaire development
The development of this questionnaire was based on modifications of annual internal patient and caregiver satisfaction surveys. All questions within these internal surveys were developed by the second author, the director of clinical services at the host university. The modifications of questionnaire reflect the change in service provision to a digital medium. Specifically, two subsections were added dedicated to (1) assessing the patient and caregiver satisfaction of telepractice and (2) comparing the satisfaction of in-person services versus telepractice. The first subsection of the telepractice satisfaction includes the patient and caregiver satisfaction of technology (e.g., “How would you rate your prior experience with Zoom before receiving telepractice at the clinic?” “How would you rate your personal technology abilities?” “How would you rate the student clinician’s technology abilities?”). In the second subsection, the original questions in the internal satisfaction survey were modified to compare the satisfaction of in-person services versus telepractice. For example, the question “please rate the student clinician’s professionalism” was modified to “the student clinician had a high level of professionalism over telepractice than in-person settings.” The question “please rate your interaction with the student clinician” was modified to “my interactions with the student clinician over telepractice were better than in-person settings.
Questionnaire content
The survey consisted of 19 questions (i.e., 17 five-point Likert-scale questions and two open-ended questions) designed to collect information pertaining to (1) the respondents’ overall satisfaction of progress, materials used in sessions, interaction with student clinicians and supervisors, and student clinicians’ professionalism regardless of service modality; (2) the respondents’ technology skills and previous experience in videoconferencing software (i.e., Zoom), and (3) preferences of service modality between telepractice and in-person modality. A full copy of the survey can be found in Appendix.
Survey distribution
The clinic’s administrative assistant distributed the Qualtrics survey via email. The Qualtrics survey was accessible for the 160 individuals from October 2020 to November 2020. The researchers decided to keep the survey open for only a month given the highly time-dependent context of the questions and the evolving nature of the pandemic. No compensation was provided for participation in this survey.
Analyses
Quantitative analyses
All survey data were analyzed with IBM SPSS Statistics (version 27). For the Likert-scale data, descriptive statistics was used to calculate means and standard deviations. A mean of one indicated that the respondent strongly disagreed or felt extremely negative. A mean of five indicated that the respondent strongly agreed or felt extremely positive. Also, t tests and Pearson correlation were used to (1) compare the respondents’ satisfaction of telepractice versus in-person services, (2) examine the relationship between the respondents’ technology skills and their satisfaction of telepractice, and (3) investigate the association between the respondents’ perception of graduate clinicians’ technology skills and their satisfaction of telepractice. Sullivan & Artino [17] and de Winter & Dodou [18] provided a rationale for the use of t tests for pairwise comparisons of Likert-scale data. Reasons supporting the use of t tests included that parametric tests such as t tests are generally more robust than non-parametric tests even when statistical assumptions (e.g., a normal distribution of data) are violated. Parametric tests are robust to yield unbiased answers when analyzing Likert-scale responses or ordinal data [17]. For five-point Likert-scale items, the t tests (i.e., parametric test) and Mann-Whitney-Wilcoxon (i.e., non-parametric test) have equivalent power for pairwise comparisons [18]. Moreover, using non-parametric methods can result in a loss of information when Likert-scale responses with high response rates are analyzed [19].
Qualitative analyses
Qualitative content analyses were completed for (1) Question 6 (i.e., would you recommend XXXXX University Speech and Hearing clinic to your friends and/or family? Why or why not?); and (2) Question 18 (i.e., is there anything that would improve your telepractice experience at the XXXXX University Speech and Hearing Clinic?). A simple categorical content analyses sort [20] was utilized for the analyses of the two above questions. The survey respondents’ open-ended responses for Questions 6 and 18 were grouped by categories and tallied. The researchers individually grouped and tallied the responses. The researchers reached 100% consensus in categories and tallies because the responses were objective and discrete.
RESULTS
Quantitative analyses
Of the 160 individuals who received the Qualtrics survey, 70 respondents (33 patients and 37 caregivers) responded to the Qualtrics survey. The response rate for this survey was 43.75%, which is within the 60±20% recommendation by Baruch [21]. Patients’ age ranges and areas of services are found in Tables 1 and 2, respectively. Among the 70 respondents, 24 received in-person services only, 13 received telepractice only, and 33 received both in-person services and telepractice. Table 3 displays demographic characteristics of survey respondents. Table 4 depicts a list of four Likert-scale questions given to all respondents (n=70) and means and standard deviations. Descriptive data indicated that the respondents were largely satisfied with the (1) progress made at the clinic, (2) quality of the student clinicians’ materials (e.g., photos, communication boards), (3) interaction with student clinicians, (4) student clinicians’ professionalism (e.g., communication skills), and (5) interaction with supervisors, regardless of service modality (M range=4.6–4.83; SD range=0.05–0.08). Table 5 exhibits a list of seven questions given to the respondents who received both telepractice and in-person services (n=33) and means and standard deviations. Thirty-three respondents who received both telepractice and in-person services did not indicate a preference between telepractice and in-person services in terms of (1) progress, (2) graduate students’ comfort level in service offering, (3) effectiveness of materials used in sessions, (4) interaction with student clinicians and supervisors, (5) graduate students’ professionalism, and (6) overall satisfaction (M range=2.85–3.39; SD range=0.14–0.22).

Patients’ age ranges (n=70)
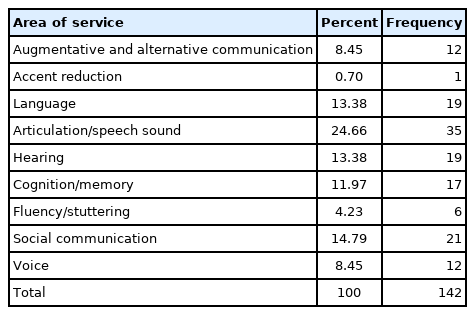
Areas of services for the patients (n=70)

Demographic characteristics of survey respondents (n=70)

Likert-scale questions and descriptive data from all respondents (n=70)
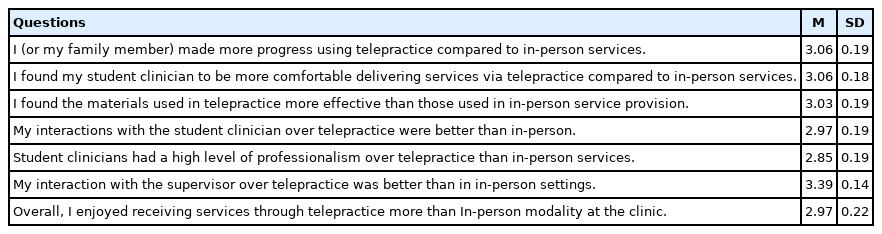
Likert-scale questions and descriptive data from the respondents who received both telepractice and in-person services (n=33)
Table 6 presents a list of four questions given to the respondents who received telepractice (n=46) and means and standard deviations. The respondents who received both telepractice and in-person services (n=33) and who received telepractice only (n=13) responded to the four questions. Descriptive data indicated that the respondents highly rated the graduate students’ technology abilities (M=4.80; SD=0.07) and overall telepractice services provided by the graduate clinicians (M= 4.59; SD=0.12). It was also found that the respondents felt positive about their prior experience with Zoom before receiving telepractice at the university clinic (M=3.87; SD=0.19) and their personal technology abilities (e.g., sharing screen and troubleshooting; M=4.11; SD=0.14). Table 7 displays one question given to the respondents who received in-person services (n=59) and means and standard deviations. The respondents who received both telepractice and in-person services (n=33) and who received in-person services only (n=24) responded to the question. Results indicated that the respondents were largely satisfied with the overall in-person services provided by the graduate students (M=4.84; SD=0.05).


One-tailed pairwise t test indicated that the respondents rated the overall in-person services significantly higher than the overall telepractice (t=2.038; p=0.022). Pearson correlation reported that the respondents’ prior experience with Zoom (r=0.120; p>0.05) and perceived technology skills (r=0.264; p>0.05) were not significantly related to their satisfaction of telepractice. However, the graduate clinicians’ perceived technology skills (r=0.322; p=0.03), professionalism (r=0.610; p<0.000), and the quality of materials (e.g., photos and communication boards) used in sessions (r=0.545; p< 0.000) were significantly associated with the respondents’ satisfaction of telepractice. Also, the respondents’ interaction with graduate students (r=0.742; p<0.000) and supervisors (r= 0.466; p=0.001) was significantly related to their satisfaction of telepractice.
Qualitative analyses
For the open-ended response, a simple categorical content analyses sort [20] was used to examine patients’ and caregivers’ satisfaction of telepractice. First, all respondents (n=70) were asked to answer whether they would recommend the university clinic to their friends and/or family (Question 6). All respondents were satisfied with the overall services provided by the university clinic. Related quotes in the responses included:
“Yes, I would recommend it to friends and family. I received an excellent hearing analysis.”
“Yes, excellent service for those who need it and can’t get through their insurance.”
“Yes, I would recommend the services at XXXXX University. In the last 13 years since my stroke in 2007, they have help[ed] me from exercises to improve mouth/tongue to reading out loud. I believe that my articulation has been improved dramatically. XXXXX University has given me too many tools in the last 13 years. I am extremely grateful for the hard work that each graduate student put in.”
Next, the respondents who received telepractice (n=46) were asked to answer whether there was anything that would improve their telepractice experience at the university clinic (Question 18). Among the responses, four themes emerged: (1) pediatric clients’ attention and behavior issues, (2) internet and technology issues, (3) convenience of telepractice, and (4) specific comments on how to improve telepractice delivery.
Theme 1: pediatric clients’ attention and behavioral issues
Caregivers of young children, especially children with attention and behavioral issues, reported that maintenance of attention in telepractice is challenging compared to the traditional in-person sessions. Related quotes in the responses included:
“My child has difficulty sitting still in front of the computer.”
“It is very difficult to keep my two-year-old daughter’s attention during Zoom.”
“My child seemed to do better in the clinic than via telepractice.”
“I think this is a difficult situation for young children.”
“Telepractice is very difficult for the age range of my daughter (5) and her goals.”
“Although I love that you are offering telepractice during this time, it is very difficult to keep my two-year-old daughter’s attention during Zoom. I know XXXXXX University is closed right now due to Covid, but I really hope that as soon as it opens back up, you will consider giving parents the option if they would be comfortable sending their child back to face-to-face. I know I would be. My daughter also goes to YYYYYY [a private practice providing speech and language services] and they have opened back up for in-person services starting in August. I feel like she got way more out of it in-person that through telepractice. She has suspected CAS, and it is hard to do motor planning mouth exercises over Zoom.”
Theme 2: internet and technology issues
Respondents indicated difficulties using videoconferencing hardware and software tools and network connection. Related quotes in the responses included:
“Not really. I had some issues with my internet speech [speed] in the spring which made it difficult to be as effective as it could have been. No fault of XXXXX University.”
“Pop is old-school, and it took him awhile to get used to the telepractice experience.”
“If I had a better computer.”
Theme 3: convenience of telepractice
Respondents indicated their preference of videoconference-based telepractice to the conventional in-person services due to their personal circumstances. Related quotes in the responses included:
“Please continue telepractice therapy. I work full time, and this works perfectly for our family.”
“Telepractice works best in the evenings for my family. I am also caring for my aging mother and have no one to bring my husband during the day while I am at work. The person at home during the day could not bring both of them to the visits.”
Theme 4: specific comments on how to improve telepractice delivery
Respondents provided the researchers with specific suggestions on how to improve or maintain the quality of telepractice delivery. Related quotes in the responses included:
“Continue to email what the session will cover prior to the Zoom. This helps parents prepare and get familiar with the iPad [augmentative and alternative communication device].
“Yes, I think give them longer time (session).”
“Yes, having more sessions. Although I felt much better, constant meetings would be even more beneficial. I am willing to pay for those meetings.”
“Perhaps giving the chance to use different media, like FaceTime, etc., because sometimes it [is] hard to connect with an unknown service.”
Other responses
Respondents also provided a variety of comments that were not included into the above four themes: (1) general satisfaction of telepractice provided, (2) general complaints of telepractice provided, and (3) specific complaints of clinicians and supervisors.
“Our current therapist [in fall 2022] is much better than our summer therapist [in summer 2022].”
“For the light to keep!”
“No, [but] so much more progress was made face to face.”
“No, everyone was incredibly kind and professional.”
“Go back to in-person. Teletherapy is brutal, too many distractions.”
“I am satisfied with the experience.”
“Getting the evaluation sooner then [than] I did. I did not receive it until after therapy for the summer was over.”
“I misunderstood the purpose of this survey. It seems your main goal is to compare remote versus in-person models, and not to get feedback on the service provided. I feel that should have been a component too in this survey. For me, the supervisor interaction was never there in summer. Fall 2019 was absolutely better experience and spring 2020 too because of students’ personality and dedication. The low scores for summer 2020 are not because of remote pattern, they are due to lack of better teaching agenda followed in summer.”
“I think clinician did wonderful job accessing his interest level and modifying assignment.”
“It would be nice for caregivers of small children to be able to watch or view the session. Perhaps from a room with closed circuit TVs. I handed off my child and did not witness interactions. My child’s skills improved, but I don’t know what they were doing.”
“No, everything was positive and very well done.”
“All good.”
“It is as good as in-person.”
“No, but it has been difficulty [difficult] for him to adapt to the telepractice after having face to face. I see improvement over time with him understanding the telepractice but still a little confusion to him.”
“I believe everyone is doing a wonderful job. Incorporating a variety of more simple games, videos, or boom cards during a session to make it more fun for the student may help.”
“No.”
DISCUSSION
Due to the COVID-19 pandemic across the globe, speech-language pathology graduate students and their clinical supervisors were required to rapidly convert clinical service delivery from in-person modality into videoconference-based telepractice. The current pilot survey study aimed to examine patient and caregiver satisfaction regarding telepractice versus in-person services provided at a university speech, language, and hearing clinic. Furthermore, the relationship between survey respondents’ satisfaction of telepractice and graduate students’ competencies in telepractice was explored. This survey study’s findings attempted to advance our understanding of telepractice-based services by analyzing patients’ and caregivers’ satisfaction of videoconference-based services. These findings also added to the limited literature of preservice telepractice instruction by identifying strengths and weaknesses of graduate students’ service delivery from the patient perspective.
Quantitative and qualitative analyses revealed that patients and caregivers were largely satisfied with the overall speech, language, and hearing services provided by graduate students at the university clinic regardless of the modality. Patients and caregivers felt extremely positive or positive about the progress made at the clinic, the quality of the graduate students’ therapeutic and diagnostic materials, interaction with the graduate students and supervisors regardless of the modality. The patients and caregivers who received telepractice rated their and graduate students’ technology skills highly. Patients and caregivers rated the overall in-person services significantly higher than the overall telepractice. Graduate students’ perceived technology skills, professionalism, quality of materials used in sessions, and interpersonal skills were identified as the predictors of patient and caregiver satisfaction of telepractice.
Telepractice-based services
Overall, patients and caregivers rated the services provided by graduate students higher for conventional in-person services compared to services delivered via telepractice. Interestingly, patients and caregivers who received both telepractice and in-person services did not demonstrate a preference between the two delivery methods. This group further observed no difference in perception of graduate student comfort, material effectiveness, clinician interaction, and observed professionalism between the two modalities. These findings are consistent with previous studies. Overall, patients were largely satisfied with service delivered via telepractice [11,13], though is not universally the preferred modality of clinical service delivery [9,14].
One factor that may explain some of the respondents’ preferences of in-person services over telepractice may be attributed to attention and behavior issues of pediatric patients found in the qualitative analyses. The caregivers of young patients expressed concerns that their child had difficulty sitting still in front of computer and paying attention to virtual stimuli. A transition from direct one-on-one intervention with the child only to family-implemented coaching and collaborative consultation under Part C of Individuals with Disabilities Education Act (IDEA) may be a great strategy to address the caregivers’ concerns in telepractice [22]. In consultation with the caregiver, graduate students can identify learning opportunities within the child’s natural environments, teach therapeutic techniques to embed within daily routines, and coordinate care via telepractice [23]. Studies have demonstrated promising results in the efficacy of coaching and collaborative consultation via telepractice in young children with communication and related disorders. For example, service coordinators, telepractice clinicians, and program administrators indicated that telepractice services strengthen family engagement and the use of coaching practices [24]. It would be of critical importance to continue research in coaching and collaborative consultation via telepractice as an effective strategy for young children with communication and related disorders.
Preservice telepractice instruction
Quantitative analyses indicated that patients’ and caregivers’ perceptions of their graduate students’ technology skills, professionalism, quality of materials used in sessions, and interpersonal skills were significantly related to overall telepractice satisfaction. It should be noted that faculty, speech-language pathology graduate students, and telepractice clinicians also ranked interpersonal skills, technology skills, and appropriate selection and preparation of online materials as the most crucial components for preservice telepractice instruction [16]. Qualitative analyses revealed respondents’ concerns pertaining to young patients’ attention and behavior issues. Overby’s [16] survey data also supported the importance of behavioral management skills in preservice telepractice training. The current survey data from patients and caregivers suggest preliminary ideas in telepractice pedagogy. Effective preservice telepractice instruction may include interpersonal skills, technology skills, appropriate selection and preparation of online materials, and behavioral management skills via clinical and academic training.
Limitations
While the study’s findings presented an initial viewpoint on telepractice service delivery, several limitations must be considered. First, the patients and caregivers who have their own hardware, software, and peripheral devices as well as internet service were only invited for telepractice due to the limited resources that the university clinic has. The researchers assumed that the patients and caregivers who felt comfortable about videoconferencing skills have received telepractice, which possibly skewed the respondents’ satisfaction. Second, the university speech, language, and hearing clinic has provided in-person and telepractice services at no cost. It is possible that respondents might be biased in their responses while receiving in-person and telepractice services free of charge that would usually be at a cost to patents and caregivers. Finally, due to the limited sample size, this study serves as a pilot to identify patient and caregiver satisfaction regarding telepractice versus in-person services. As a result, patients’ and caregivers’ data were combined for analyses. Considering the evidence indicating the discrepancies between patient versus caregiver satisfaction of telepractice [14], separate examinations in patients’ and caregivers’ responses could have led to more accurate interpretation of satisfaction data. Furthermore, various confounding variables (e.g., age, gender, severity of communication difficulties, type of communication disorders, and frequency and duration of treatment sessions) and their interaction that potentially affect service satisfaction have not been measured and analyzed [10,13]. Further investigation is recommended to determine the main and interaction of the confounding variables on patient and caregiver satisfaction regarding telepractice versus in-person services.
Directions for future research
In conclusion, the current pilot study attempted to extend our understanding of videoconference-based telepractice services and clinical education by surveying patients’ and caregivers’ satisfaction. The findings highlighted the significance of adopting telepractice clinical and technical skills in preservice instruction. It is essential for university faculty and clinical supervisors to put more efforts into developing better preservice academic and clinical training in telepractice service delivery. Patients’ and caregivers’ satisfaction data suggested important aspects for graduate curriculum such as interpersonal skills, technology skills, appropriate selection and preparation of online materials, and behavioral management skills via clinical and academic training. Future studies are necessary to directly observe the effect of telepractice-based clinical and academic training on speech-language graduate students’ competencies in telepractice. Evaluating patients’ data versus caregivers’ data separately is also suggested because differences in the satisfaction data have been reported.
References
Appendices
Survey of Patient and Caregiver Satisfaction of Services Provided at a University Clinic
cacd-2021-00598-Appendix-1.docx