


INTRODUCTION
Aphasia is a condition that poses significant language impairment due to brain injury, usually present in the left hemisphere of the brain, commonly due to stroke [1]. The condition presents with impairments in comprehension, expression, naming, reading, and writing. Out of these impairments, word retrieval deficits or anomia is debilitating and ubiquitous among discrete variants of aphasia [2]. Assessment of anomia in the clinical setting plays an imperative role to categorize different variants of aphasia.
Further, aphasia is a multifaceted condition present with a discrete and wide array of Linguistic deficits and these deficits may vary among the same type of aphasia. Hence, as Speech Language Pathologist, it is important to note these variations among each type of PWAs and apply the appropriate treatment protocol suiting the individual. In addition, among the constellation of linguistic impairments possessed by PWAs, word retrieval deficits (anomia) seem pervasive and more distressing among PWAs.
These word retrieval deficits cause significant impact at a single word level, sentence level, and discourse production [2]. This significant breakdown at various levels could occur due to the inability to access the semantic network or impairment at the semantic network or impairment at the phonological level in general. In addition, the errors are further categorized as semantic paraphasias (‘pen’ for ‘pencil’), phonemic paraphasias (‘wencil’ for ‘pencil’), and neologisms (‘mogo’ for ‘dog’).
Documenting the type of error patterns may aid in pinpointing the source of errors (semantic or phonological level). Change in error patterns following treatment signifies strengthened semantic networks and increased activation for word retrieval [3]. Owing to the aforementioned strengths of appraising errors in PWAs following treatment, the current study designed a treatment protocol named Semantic Cueing of verbs and its thematic role (SCVTr). This protocol uses verbs as their pivotal stimuli and expands their semantic knowledge using thematic roles (agent/patient) around the verbs. These exercises provide an opportunity for a wide array of activation of the semantic networks and, in turn, spread the activation to the neighbouring networks. Thus, the activation may aid in enhancing the corpus of words [4].
Need for the study
Error analysis technique aids in understanding the psycholinguistic mechanisms associated with word retrieval. In addition to the linguistic test scores, if authors document the change in errors following treatment it may give better insight into the prognosis of PWAs. For instance, to claim a good prognosis, the PWAs should display a decrement in semantic or phonemic errors, which might suggest that there is a widespread activation of the semantic network [3,5]. Despite the significance of error analysis, most of the study outcomes elucidate the improvement merely in assessing the accuracy of naming skills. Thus, the present study was designed to assess the error patterns following the treatment.
METHOD
Participants
In the current study, sample size was estimated using G* power software version 3.1 [6]. The difference in mean and standard deviations for the outcome measure was derived for the first four participants of the study. The outcomes served as the input to the G* power software, and the analysis prescribed the sample size ranging from three to ten. Thus, the present study recruited total of 11 PWAs. These PWAs were inclusive of both fluent and non-fluent variants with minimum of six-month post- stroke were enrolled for the study. These PWAs average age was 38.72 years (Range=24–64, SD=11.97) recruited from in around Mysuru district via convenient sampling method. (Table 1)
The participants recruited for the study should be right handed prior to CVA; should be native speaker of Kannada; should poses normal hearing and normal vision/corrected vision; and should be free from other degenerative neurological conditions and psychiatric conditions. In addition, the participants were rule out for comprehension and Apraxia of Speech deficits using WAB-K.
Materials
These participants were assessed for identifying, categorizing the type of aphasia and evaluating word retrieval deficits via Western Aphasic Battery in Kannada (WAB-K) [7]; Action Naming Test (ANT) [8]; and Boston Naming Test (BNT) [9]; The aforementioned tests were scored as per the standard scoring in the manuals.
Procedure
The PWAs were appraised for trained and untrained probes at three phases namely, pre-treatment phase, treatment phase, post-treatment phase, and follow-up phase. Assessment of trained and untrained probes were carried out only at pre-treatment phase, post-treatment phase, and follow-up phase. Further, in order to avoid exposure effect counterbalancing of the stimuli was done.
At pre-treatment phase, trained probes contained verbs (e.g.,/pujisu/) and their related thematic role (e.g.,/pujari/-/devaru/). Trained probes were assessed via pictures for both verbs and their thematic role. If PWAs were unable to retrieve the desired words, then semantic cues followed by phonemic cues were rendered. Scoring of responses followed a ‘four-point rating scale, where score ‘three’ referred to words retrieved without any cues; score ‘two’ if the participants gave the desired response with a semantic cue; score ‘one’ if the participants gave the desired response with a phonemic cue; and score ‘zero’ referred to no retrieval even with the cues. Untrained probes were assessed via pictures for verbs, and PWAs were instructed to construct the plausible thematic roles based on their discretion. Assessment of untrained probes followed a scoring pattern of ‘zero’ and ‘one’; where score ‘zero’ referred to erroneous production and score ‘one’ referred to correct word retrieval. Similar stimuli and procedure was followed at post-treatment and follow-up phase. in this study, follow-up phase was assessed after one month of cessation of treatment. In this study, only erroneous response was further considered for analysis.
At treatment phase, SCVTr treatment was rendered; where PWAs were presented with 10 target verbs with a range of minimal (broad cues) and maximal cues (narrower cues). Based on the success of the retrieval minimal to maximal cues were presented. Irrespective of the success in the verb retrieval, PWAs were solicited for generating plausible thematic roles. Minimal to maximal cueing strategy was followed when PWAs were unable to retrieve. After the generation of verbs and their thematic roles, they were instructed to read aloud. If PWAs were unable to repeat, then the researcher employed choral reading. ‘Wh’ questions on verbs and their thematic roles were posed, if PWAs failed to answer then choices were presented; sentences generated with verbs and their thematic role were semantically judged. Finally, PWAs were instructed to construct the verbs and their thematic role independently. If PWAs were unable to retrieve the words independently, then the researcher read the response for PWAs. The SCVTr treatment protocol was rendered for a minimum of ‘two’ sessions and a maximum of ‘three’ sessions. The treatment continued until PWAs reached the 80% criterion [10]. The accuracy scores of word retrieval was not considered in the present study, as this was published as phase one study [4].
Data analysis
The verbatim of trained and untrained stimuli (probes) of the pre-treatment phase, post-treatment phase, and follow-up phase were subjected to error analysis using Edmonds et al. protocol [3]. Error responses were categorized as
A semantic error: Substitution of semantically related word for the target word (Cat for Dog).
Phonemic error: Substitution/ deletion/ insertion of other phonemes (Bog/Do/Doggi for Dog).
Mixed error: The target word is both semantically and phonemically related (Rat for Cat).
Unrelated: Substitution of words which are neither semantically or phonemically related tothe target word (Mat for Dog).
Neologisms: Substitution of non-word (non-meaningful word) for the target word (Mogo for Dog).
I Don’t Know (IDK)/ No response: Absence of response for the target word.
Perseveratory error: Inappropriate reoccurrence or repetition of previously produced or heard responses.
All the error response was audio-video recorded across the different phases of the study. This response was qualitatively assessed among each participants.
RESULTS
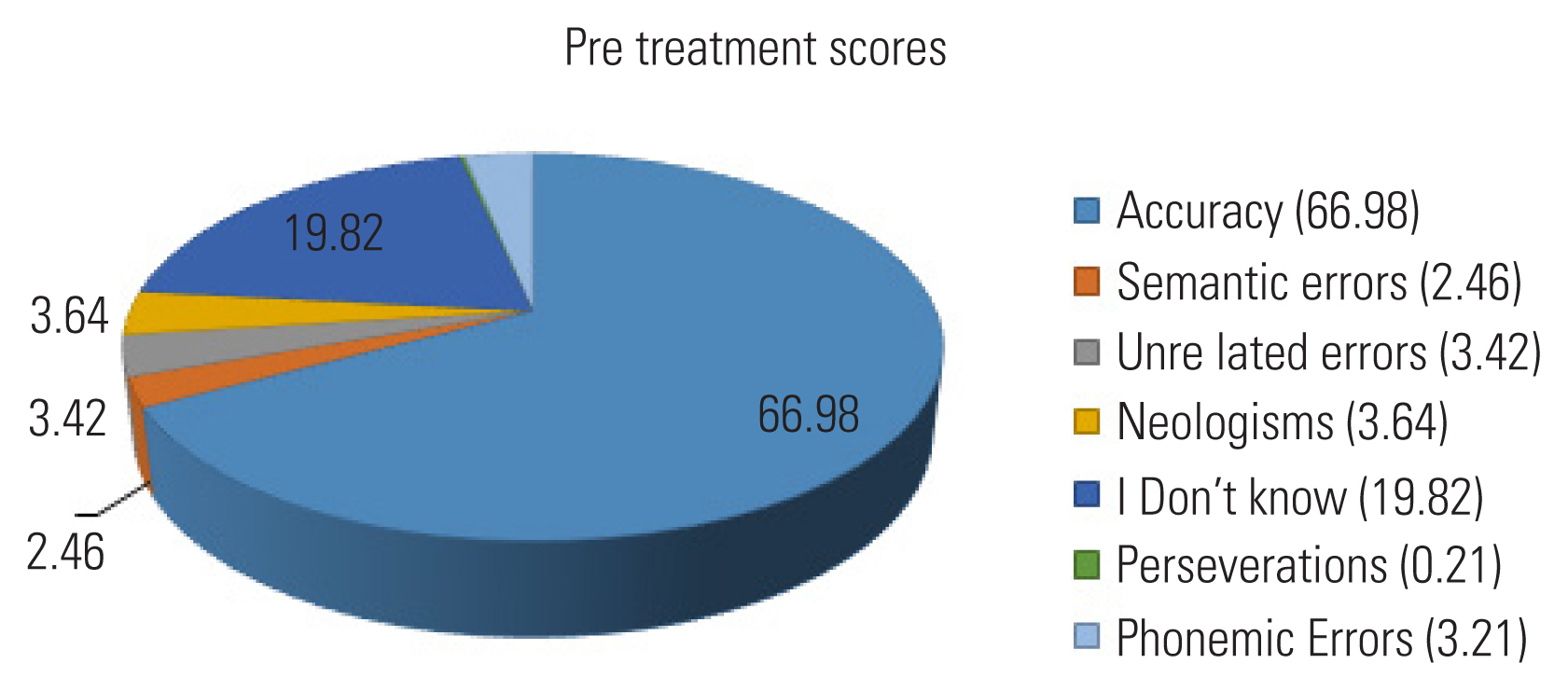
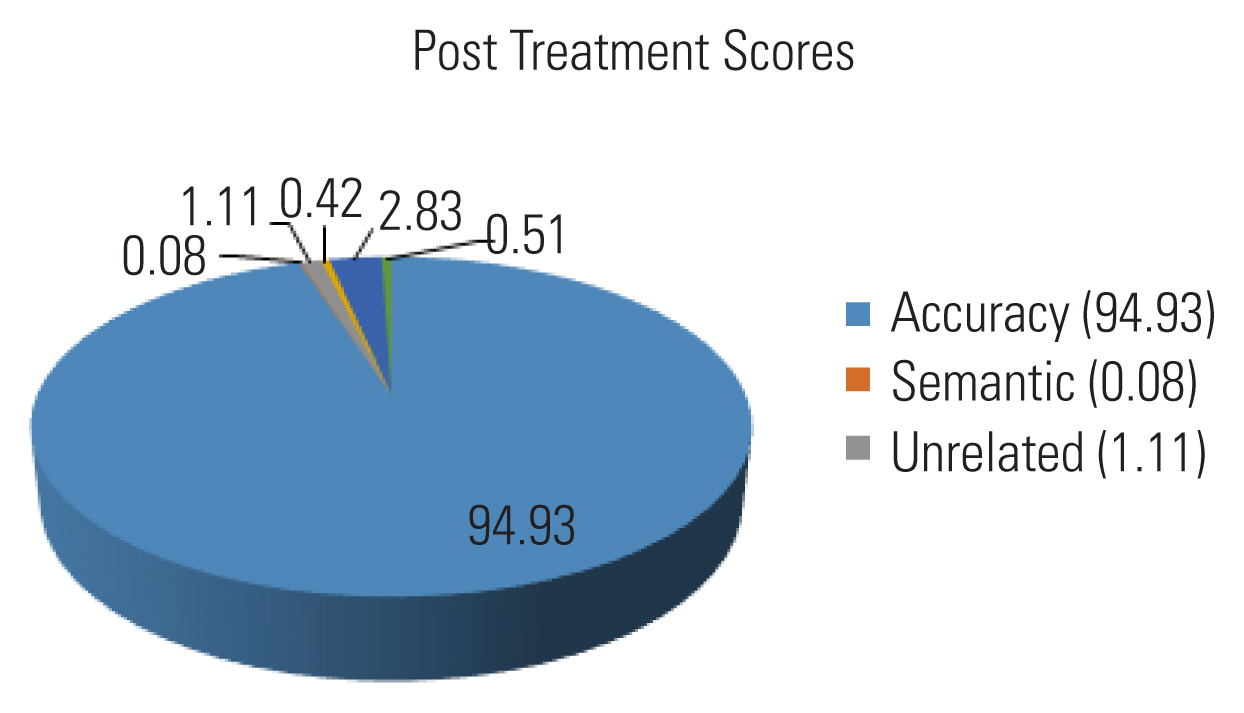
On addressing the objectives ‘one’ and ‘two’, the errors patterns exhibited by all the participants in the pre-treatment phase were; ‘IDK’ (I don’t know) or No response (NR) (19.82%) were maximally produced, followed by Neologisms (NE) (3.64%), Unrelated (UR) (3.42%), Phonemic errors (PE) (3.21%), Semantic errors(SE) (2.46%) and Perseverations(PER) (0.21%) (IDK> NE>UR>PE>SE>PER) (Figure 1). On measuring error patterns of trained and untrained spoken stimuli at the post-treatment phase, the preponderance of errors were ‘IDK’ (2.83%), followed by UR (1.11%), PE (0.51%), NE (0.42%), and SE (0.08%) (IDK>UR>PE>NE>SE). On comparing pre to post-treatment phases, all the errors were markedly reduced. (Figure 2) Raw scores of all PWAs were documented in Table 2. Further, the error scores of each PWAs across pre, post, and follow-up phase were also documented. (Table 2)
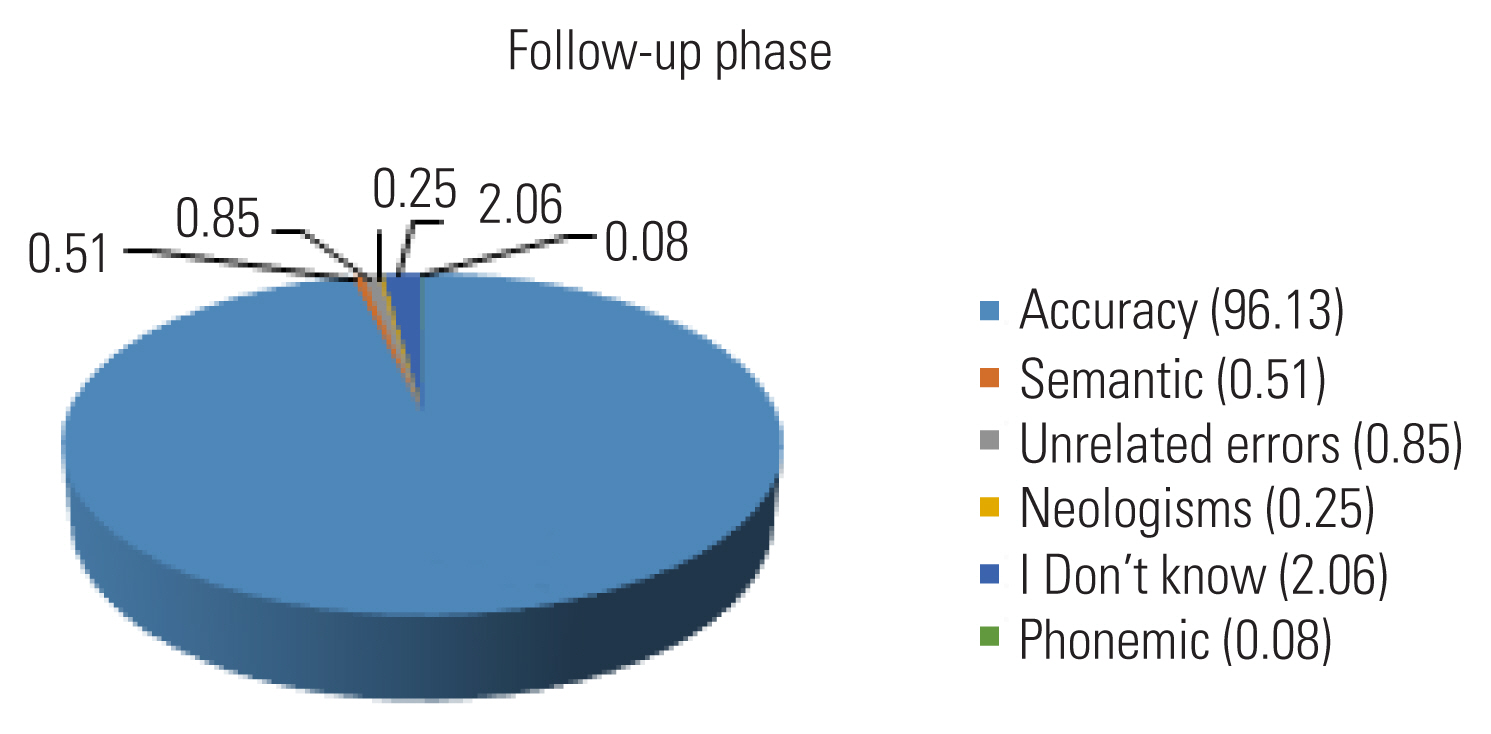
On computing the total errors in the follow-up phase, predominantly IDK (2.06%) was highest, followed by UR (0.85%), SE(0.52%),NE (0.25%) and PE (0.08%) (IDK>UR>SE>NE>PE).
On comparing the errors from the post to the follow-up phase, the UR and NE did not vary. However, the IDK and PE errors manifested a decrement in the frequency of errors at the follow-up phase. Furthermore, SE was perceptibly high in the follow-up phase compared to the post-treatment phase. (Figure 3)
To summarize, the errors patterns of individual participants across pre and post-treatment phases showed alleviated scores at the post-treatment phase among all the participants. Furthermore, all the participants exhibited almost identical error score pattern at the follow-up phase as in the post-treatment phase. The participants P1,P7,P8, and P11 showed overall reduction in different types of errors from pre to post-treatment phase. These participants manifested errors such as ‘IDK’, NE, UR, PE, and SE that reduced from pre to post-treatment phase. In addition, the participants P1,P7,P8, and P11 manifested same error pattern at the follow-up as in the post-treatment phase.
In P2, the overall errors reduced from pre to post-treatment phase. Wherein, P2 exhibited reduction in errors such as ‘IDK’, PER, NE, PE, and UR errors. On measuring errors at the follow-up phase, P2 evinced similar error scores as in the post-treatment phase. In P3,P5 and P9, the overall errors reduced from pre to post treatment phase. Errors noted for these participants were ‘IDK’, UR, and SE. Further, these errors reduced individually from pre to post-treatment phase. The computed error scores were maintained from post to follow-up phase.
P4 showed overall reduction in errors from pre to post-treatment phase. The errors manifested by P4 were ‘IDK’, NE, UR, PE, PER, and SE these errors reduced from pre to post-treatment phase. Also, the participant P4 showed same error pattern at the follow-up phase as in the post-treatment phase.
In P6, the overall errors reduced from pre to post-treatment phase. Errors demonstrated by participant P6 showed reduction in ‘IDK’, PE, NE, and UR. Concurrently, on measuring errors at the follow-up phase, an identical pattern was noted as in the post-treatment phase. In P10, the overall errors reduced from pre to post-treatment phase. The errors exhibited by P10 were ‘IDK’, PE, UR, and SE. Subsequently, P10 evinced identical error pattern at the follow-up phase as in the post-treatment phase. (Table 3).
DISCUSSION
Analysing the evolution of errors following word retrieval treatment seems an intriguing phenomenon, as this pinpoints the origin of the errors. Based on the origin of errors, errors can be categorized into semantic error, phonological error, neologism, and no response. This information seems imperative as it posits the improvement of a particular approach over the course of treatment. Despite its pivotal role in claiming the prognosis, a majority of the word retrieval treatment studies failed to document changes in errors over the course of treatment. However, a handful of studies document the evolution of errors in the previous VNeST related studies [11,12].
The evolution of error patterns over the course of treatment, advocate that there is an increased processing during lexical retrieval among all participants across the treatment phases. To elaborate, the error patterns among all the participants across pre and post-treatment phase were as follows: semantic errors markedly decreased from ‘23’ to ‘1’; unrelated errors reduced from ‘32’ to ‘13’; neologisms alleviated from ‘34’ to ‘5’; “I Don’t know” showed decrement from ‘185’ to ‘33’; perseveration reduced from ‘2’ to ‘0’; phonemic errors reduced from ‘30’ to ‘6’. Thus, from the overall error patterns documented, it can be claimed that there was a marked reduction in errors from pre to post-treatment phase among all the participants.
Semantic errors exhibited by the participants indicate inaccurate or incomplete activation of semantic representations of the target items. The semantic errors usually co-occur with comprehension impairments [13]. There are other case reports which opined semantic errors could have a post-semantic origin. The participants with this origin exhibited intact comprehension abilities with concomitant semantic errors on oral or written production tasks [14,15]. In addition, occurrences of semantic errors were predicted due to inaccessibility to the phonological representations, thereby resulting in highly activated semantically related errors instead of phonological counterparts. An alternate explanation proposed by literature on the production of semantic paraphasia is that semantic paraphasia is interpreted as “noise” at the level of the lexical-semantic node; due to this, there is activation at the neighboring semantic nodes instead of the target word [14,15]. These explanations are in support of the presence of semantic errors noted in the present study.
The presence of unrelated errors in the current study can be attributed to remote activation of lexical representations instead of target lexical representations. Hence, there is a high tendency of retrieval of more readily accessible lexical representation resulting in unrelated responses. Also, in the word retrieval process, a large array of semantic networks may be activated. In order to successfully retrieve the target word, that word should gain the required threshold. If participants fail to reach the required threshold for the target word then, the word which attains the threshold instantly might be retrieved, resulting in unrelated responses. These explanations are in consensus on comparing the present study results to the study by Hashimoto [5].
Neologisms were evinced in the present study; however, these errors were markedly reduced from pre to post-treatment phase. The presence of neologisms was due to failure or difficulties during lexical retrieval [16]. Further, this error can result from impairment in connections at various levels. To elaborate, errors could result from impairment in the connections between the semantic system and lexical system, impairment within the lexical system, and impairment in the connection between the lexical and phonological systems. The neologisms could result from a combination of the impaired processes as alluded earlier or impairment in isolation [12].
During the evaluation of errors, all participants exhibited “I don’t know” (IDK) or No response (NR) suggesting a failure in accessing the target lexical representations of any form (semantic or phonological). Also, if the participant exhibits ‘IDK’ responses, it can be posited that the activation occurring at the semantic level is minimal or absent. Thus, results in having less number of lexicons for retrieval or present with no lexicon at the time of word production. In other instances, activation might occur at the semantic level but fail to cascade the activation to lexical-semantic or phonological level due to weak connections among these levels.
Analysis of errors among all the participants showed phonemic errors in pre and post-treatment phases. However, these errors were markedly reduced from pre to post-treatment phase. This error could be asserted due to the impairment at lexical-phonological or post-lexical phonological output buffers. Errors that originate at the lexical-phonological level could be resulting from impairment at retrieval of stored lexical–phonological information. Subsequently, the phonological errors that are distant from the target word imply that more readily available phonological forms were used to retrieve the word. However, more closely resembling phonological form to the target word would be due to post-lexical processing-level deficits [5]. Additionally, the phonological error may arise due to increased word length [17].
Perseveration was also noted among all the participants in the study, but with minimal occurrence relative to the other errors as aforementioned. The presence of perseveration can also be explained subsequently to the deficit in post-lexical processing. Due to this, there are several attempts of self-corrections secondary to awareness of incorrect activation of phonological representation. Yet another elucidation for the occurrence of perseveration might be due to the inability to inhibit the semantic networks activated around the target word, indicating weak connections associated with the semantic networks. Thus, it results in perseverations [5].
The overall evolution of errors across pre and post-treatment phases was investigated. The pattern of error evidenced in the pre-treatment phase was IDK>NE>UR>PE>SE>PER, whereas the errors documented in the post-treatment phase was IDK>UR>PE>NE>SE. Wherein, error pattern slightly differed from pre to post-treatment phase. Additionally, the frequency of occurrence of each type of error decreased drastically from pre to post-treatment phase as aforementioned.
The above findings imply that the SCVTr protocol used in the study had widespread gains on potentially reducing the variants of errors among all the participants. Specifically, this can be attributed to the use of the SCVTr protocol, which is theoretically a semantic-based treatment. Thus, it aids in reinforcing a wide array of semantic networks. This protocol also entails the use of orthography and the phonological form of the target word, which further strengthens the semantic networks corresponding to the target word. This activation assists in enhancing the corpus of words, and it in-turn strengthens the connections between the semantic networks associated with the target words resulting in the reduction of the semantic errors in the post-treatment phase.
In nutshell, the change in error pattern (pre to post-treatment phase) and maintenance of error pattern in the follow-up phase can be posited due to (1) increased activation and strength in semantics and phonological connections. (2) Increased enhancement in the threshold of activation for the intended target through systematic training. (3) Strengthening connections at lexical, semantic and phonological level. (4) Alleviation of lexical retrieval failures. (5) Strengthening word retrieval process at the post-lexical level. All these aforementioned entities seem crucial in the reduction of discrete errors such as semantic errors, unrelated errors, neologisms, ‘IDK’, phonemic error, and perseverations from the pre to post-treatment phase [5,3].
Summary and Conclusions
The error analysis technique is the most powerful tool to track the changes at the psycholinguistic level. However, most of the studies fail to document the error pattern across the treatment phases. Owing to the shortfall of knowledge and due to the intrinsic nature of error patterns, the study results may shed light on fostering error analysis both in the assessment and in treatment of PWAs. This inculcation may guide the clinicians to streamline their cueing strategies accordingly.
Understanding the type of error pattern in PWAs during the assessment plays an imperative role in elucidating the loci of word retrieval deficits. The loci of word retrieval deficits can be semantic/lexical or phonemic in nature, owing to which appropriate cueing strategies can be applied in order to assess naming skills of PWAs. Documenting the error pattern during the course of treatment pave a way to SLPs to render appropriate cueing strategies in instances of inappropriate word retrievals during object naming or in discourse. Also, understanding error patterns in PWAs enables SLPs to use specific cues such as semantic or phonemic or mixed cues during therapy. This may foster better word retrieval abilities at word, sentence, and discourse levels.